
今回は、大腸がん術前のリハビリテーションの効果について調査した論文を紹介します。
以前に大腸がんの手術後にプレリハビリテーションを行った方がいいのではないかという考察を書いた論文を紹介しました。
プレリハビリテーションは手術前に体が弱らないように行うリハビリのことですが、重要そうであまり周知はできていません。
そこで今回は、大腸がん術前のリハビリテーションの効果について調査した論文を紹介します。
・術前のリハビリを行うことで、術後の結果が若干改善はしたが、統計的に有意差はでなかった。
・術前のリハビリは重要と思うが、いかに筋力や体力をアップするリハビリを提供できるかが大事だと思われる。
今回紹介する研究の概要
今回紹介する論文は、大腸がん術前のリハビリテーションの効果について調査した内容となっています。
「Lindman A, Handberg C, Olesen G, et al. Can physical prehabilitation prevent complications after colorectal cancer surgery in frail older patients? van der Hulst HC, Bastiaannet E, Portielje JEA, van der Bol JM, Dekker JWT. Eur J Surg Oncol. 2021 Nov;47(11):2830-2840. 」、2021年に発行された論文です。
家から徒歩0分のヨガスタジオ対象
This observational cohort study included all CRC patients ≥70 years who received elective surgery in a teaching hospital in the Western part of the Netherlands from January 2014 until December 2019. Patients were excluded if they were not eligible for the physical prehabilitation program; in case of non-elective surgery, metastatic disease, local excision as surgical procedure, clinical admission prior to surgery, partial obstructive tumor symptoms, and/or not able to exercise or refusal of participation.
Lindman A, Handberg C, Olesen G, et al. Can physical prehabilitation prevent complications after colorectal cancer surgery in frail older patients? van der Hulst HC, Bastiaannet E, Portielje JEA, van der Bol JM, Dekker JWT. Eur J Surg Oncol. 2021 Nov;47(11):2830-2840.
対象は、2014年1月から2019年12月までオランダ西部の教育病院で待機的手術を受けた70歳以上のすべてのCRC患者が含まれていました。
除外基準は、転移性疾患、外科的処置としての局所切除、部分的閉塞性腫瘍症状、運動できない、または参加を拒否する場合の患者さんでした。
家から徒歩0分のヨガスタジオ方法
We divided the patients in two groups: the physical prehabilitation (PhP) group and the non-prehabilitation (NP) group. Patients in the NP-group did not initiate the program, because of two reasons: 1. The program was not offered to these patients, as they were <75 years and received surgery between 2014 and 2018 and 2. The program was not offered to these patients because they were considered too fit for prehabilitation based on the clinical impression of the care professional.
The PhP-group that was based on an intention-to-treat (ITT) population consisted of all patients who initiated the program, independently of complying the whole program. The PhP-group that was based on the per protocol (PP) population consisted of patients who complied at least four weeks of the physical prehabilitation [39,54,55]. Patients who participated in the physical prehabilitation program for less than four weeks were excluded from the PP analyses.
Lindman A, Handberg C, Olesen G, et al. Can physical prehabilitation prevent complications after colorectal cancer surgery in frail older patients? van der Hulst HC, Bastiaannet E, Portielje JEA, van der Bol JM, Dekker JWT. Eur J Surg Oncol. 2021 Nov;47(11):2830-2840.
患者をプレリハビリテーション(PhP)グループと非プレハビリテーション(NP)グループに分けて、PhPグループは、少なくとも4週間の身体的リハビリテーションを遵守した患者で構成されていました[ 39、54、55 ]。
家から徒歩0分のヨガスタジオ結果
Lindman A, Handberg C, Olesen G, et al. Can physical prehabilitation prevent complications after colorectal cancer surgery in frail older patients? van der Hulst HC, Bastiaannet E, Portielje JEA, van der Bol JM, Dekker JWT. Eur J Surg Oncol. 2021 Nov;47(11):2830-2840.
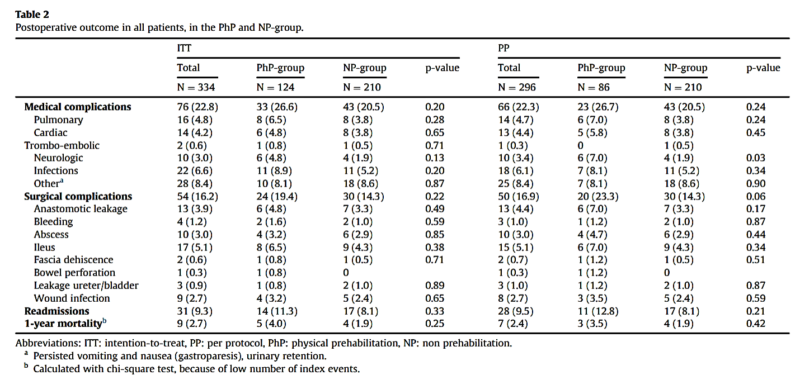
こちらの表は対象者の特性です。
診断時の年齢の中央値は75歳(IQR 73.0–81.0)で、284人(85.0%)が腹腔鏡手術を受けました。
93人(27.8%)のASAスコアはIII以上、72人(21.6%)の併存疾患は2以上と併存疾患があり、72人(21.6%)は歩行補助器具を使用して、95人(28.4%)のG8フレイルスコアは陽性でした。
PhPグループの患者は、診断時の年齢が高く(80.0 vs. 74.0歳、p <0.001)、ASAスコアが高く(ASA≥III:37.9 vs. 21.9%、p = 0.002)、併存疾患が多い(≥2併存疾患 :31.5 vs. 15.7%、p = 0.001)、歩行補助器具のより頻繁な使用(38.7 vs. 11.4%、p <0.001)および「一人暮らし」の割合が高い(46.8 vs. 32.8%、p = 0.023) ことが特徴でした。
Lindman A, Handberg C, Olesen G, et al. Can physical prehabilitation prevent complications after colorectal cancer surgery in frail older patients? van der Hulst HC, Bastiaannet E, Portielje JEA, van der Bol JM, Dekker JWT. Eur J Surg Oncol. 2021 Nov;47(11):2830-2840.

図AはNP群と比較してPhP群の方が合併症の発生率が低かったことを示しています。差は有意ではありませんでしたが、すべての虚弱なサブグループで低い合併症率のパターンが見られました。
図Bは虚弱患者の外科的合併症率がNPグループと比較してPhPグループでほとんど高かったことを示しています。
図FではNPグループと比較してPhPグループで再入院率が低いというより特徴的なパターンを示しました。
家から徒歩0分のヨガスタジオ結論
In this study, patients ≥70 years with elective colorectal cancer, who initiated or completed a physical prehabilitation program had a worse frailty profile and therefore a higher a priori risk for postoperative complications. However, with physical prehabilitation, rates of medical complications, surgical complications and readmissions were not different compared to patients without prehabilitation. This suggests that physical prehabilitation for frail CRC patients ≥70 years may prevent postoperative complications.
Lindman A, Handberg C, Olesen G, et al. Can physical prehabilitation prevent complications after colorectal cancer surgery in frail older patients? van der Hulst HC, Bastiaannet E, Portielje JEA, van der Bol JM, Dekker JWT. Eur J Surg Oncol. 2021 Nov;47(11):2830-2840.
この研究では、身体的リハビリテーションプログラムを開始または完了した大腸がんの70歳以上の患者は、虚弱プロファイルが悪化し、したがって術後合併症の先験的リスクが高かったことが明らかとなりました。
ただし、プレハビリテーションでは、医学的合併症、外科的合併症、および再入院の割合は、プレハビリテーションのない患者と比較して違いはありませんでした。
なかなか、術前のリハビリの効果を明確に出すのは難しいようですね。
印象としては、術前に筋力や体力がつけば手術成績もよくなると思うので、いかに術前に効果が出るリハビリプログラムを提供できるかが重要でしょうね。
家から徒歩0分のヨガスタジオ・術前のリハビリを行うことで、術後の結果が若干改善はしたが、統計的に有意差はでなかった。
・術前のリハビリは重要と思うが、いかに筋力や体力をアップするリハビリを提供できるかが大事だと思われる。
このブログは、ガイドラインや論文などの根拠をもとに情報を発信していく予定です。
しかし、がんの病態や治療方法によっては、お読みになっているがん患者さんにはその情報が当てはまらない場合もあります。
記事の内容を参考に新しく何かを始める場合には、担当の医師や医療従事者にご確認いただくようお願いいたします。

















最近のコメント