
今回は、四肢の骨転移に対する手術の効果について調査した研究を紹介します。
前回は頸椎転移に対する手術療法はPSやQOLを改善させるといった論文を紹介しました。

頸椎転移に対して手術療法も検討して方がいいという話でしたね。
骨転移は脊椎以外にも上腕骨や大腿骨といった四肢にも出現しやすいですが、そちらに対する手術の効果はどうなのでしょうか?
そこで今回は、四肢の骨転移に対する手術の効果について調査した研究を紹介します。
今回紹介する研究の概要
今回紹介する論文は、四肢の骨転移に対する手術の効果について調査した内容になっています。
「Hara H, Sakai Y, Kawamoto T, et al. Surgical outcomes of metastatic bone tumors in the extremities (Surgical outcomes of bone metastases). J Bone Oncol. 2021 Feb 19;27:100352 J Orthop Surg Res. 2021 Jul 3;16(1):423」、2021年に発行された論文です。日本の先生が書いた論文ですね。
47人の整体師全員が「整体対決で負けた」枕!【Cure:Re THE MAKURA】対象
This study included 114 patients (61 men, 53 women; median age, 66 [range, 22–87] years) who underwent surgery for limb and acetabular bone metastases between 2008 and 2019 in our institution. The patients were registered at operation and followed until December 2019 or death. The median duration of follow-up was 12 (range, 0–130) months. There was surgical indication for bone metastasis with severe pain and high risk of pathological fracture. In some cases, the bone metastasis was radically resected. We defined the patient’s general condition needed to be tolerable for surgery, whose expectable prognosis needed at least one month.
Hara H, Sakai Y, Kawamoto T, et al. Surgical outcomes of metastatic bone tumors in the extremities (Surgical outcomes of bone metastases). J Bone Oncol. 2021 Feb 19;27:100352 J Orthop Surg Res. 2021 Jul 3;16(1):423
対象は、 2008 年から 2019 年の間に四肢および寛骨臼の骨転移に対して手術を受けた患者 114 例(男性 61 例,女性 53 例,年齢中央値 66[範囲,22~87]歳)です。
追跡期間の中央値は12(範囲:0~130)カ月でした。
手術適応は、強い疼痛と病的骨折のリスクの高い骨転移であり、手術に耐えられる全身状態であること,予後が1ヶ月以上見込めることが条件となっています。
47人の整体師全員が「整体対決で負けた」枕!【Cure:Re THE MAKURA】方法
The patients were classified into three groups based on surgical procedures (1) the fixation group (59 cases), in which only internal fixation was performed without tumor curettage or resection; (2) the curettage group (27 cases), in which internal fixation was performed in addition to bone cement filling after intra-tumoral resection (tumor curettage); and (3) the resection group (28 cases), in which en-bloc tumor resection was followed by reconstruction using an implant.
To control for other factors affecting patient prognosis, we evaluated age, sex, presence of pathological fracture, type of primary tumor, presence of visceral metastases, presence of multiple bone metastases, history of chemotherapy, history of radiation therapy to surgical sites, surgical procedures for bone metastases, and the use of bone-modifying agents (BMA). Primary tumors were classified as three subgroups according to Katagiri score [8]. The Kaplan-Meier plot and log-rank test were used to compare overall survival for each factor. A chi-square test of independence was calculated comparing the frequency of pathological fracture in presence or absence of preoperative administration of BMA. As for 69 out of 114 cases that could be followed up for more than 6 months after surgery, we evaluated PS, ADL, QOL, and pain at 3 and 6 months postoperative relative to these preoperative values. PS was evaluated using the Eastern Cooperative Oncology Group (Zubrod, World Health Organization) performance scale. ADL, QOL, and pain were assessed using the Barthel Index (BI), EuroQoL 5 Dimensions (EQ-5D), and Numerical Rating Scale (NRS), respectively.
Hara H, Sakai Y, Kawamoto T, et al. Surgical outcomes of metastatic bone tumors in the extremities (Surgical outcomes of bone metastases). J Bone Oncol. 2021 Feb 19;27:100352 J Orthop Surg Res. 2021 Jul 3;16(1):423
1)腫瘍掻爬や切除を行わず内固定のみを行った固定群(59例)、(2)腫瘍内切除(腫瘍掻爬)後に骨セメント充填に加え内固定を行った掻爬群(27例)、(3)腫瘍一括切除後にインプラントを用いて再建した切除群(28例)に分類しています。
患者の予後に影響を与える他の要因をコントロールするために、年齢、性別、病理学的骨折の有無、原発腫瘍の種類、内臓転移の有無、多発性骨転移の有無、化学療法歴、手術部位への放射線療法歴、骨転移に対する外科処置、骨修飾剤(BMA)の使用について評価しています。
さらに、原発腫瘍は片桐スコア[8]に従って3つのサブグループに分類されています。
Kaplan-Meierプロットとlog-rank検定を用いて、各因子の全生存期間を比較しました。
術後6カ月以上経過した114例中69例について,PS,ADL,QOL,疼痛を術前値と術後3カ月,6カ月で相対評価した。PSはEastern Cooperative Oncology Group(Zubrod、世界保健機関)のパフォーマンススケールを用いて評価した。ADL、QOL、痛みはそれぞれBarthel Index(BI)、EuroQoL 5 Dimensions(EQ-5D)、Numerical Rating Scale(NRS)を用いて評価しました。
47人の整体師全員が「整体対決で負けた」枕!【Cure:Re THE MAKURA】結果
Hara H, Sakai Y, Kawamoto T, et al. Surgical outcomes of metastatic bone tumors in the extremities (Surgical outcomes of bone metastases). J Bone Oncol. 2021 Feb 19;27:100352 J Orthop Surg Res. 2021 Jul 3;16(1):423

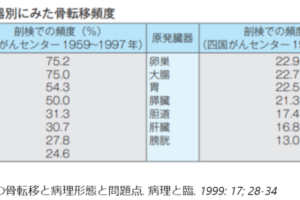
こちらは対象者の原発巣です。
原発巣の種類は腎癌が最も多く、次いで肺癌、甲状腺癌、乳癌です。
骨転移の手術部位は、上肢33例、骨盤周囲51例、非骨盤周囲下肢30例(寛骨臼5例、その他25例)でした。
47人の整体師全員が「整体対決で負けた」枕!【Cure:Re THE MAKURA】Hara H, Sakai Y, Kawamoto T, et al. Surgical outcomes of metastatic bone tumors in the extremities (Surgical outcomes of bone metastases). J Bone Oncol. 2021 Feb 19;27:100352 J Orthop Surg Res. 2021 Jul 3;16(1):423
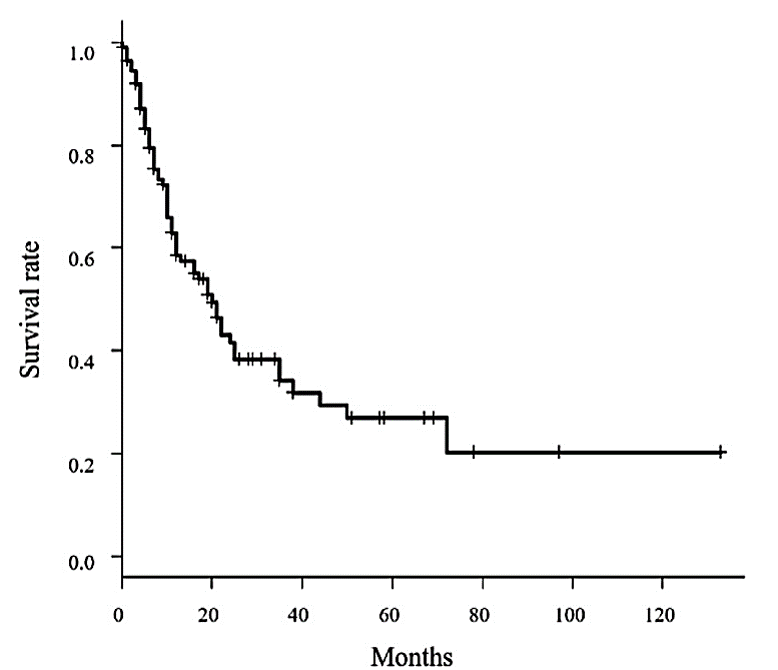
こちらは生存期間のグラフになります。
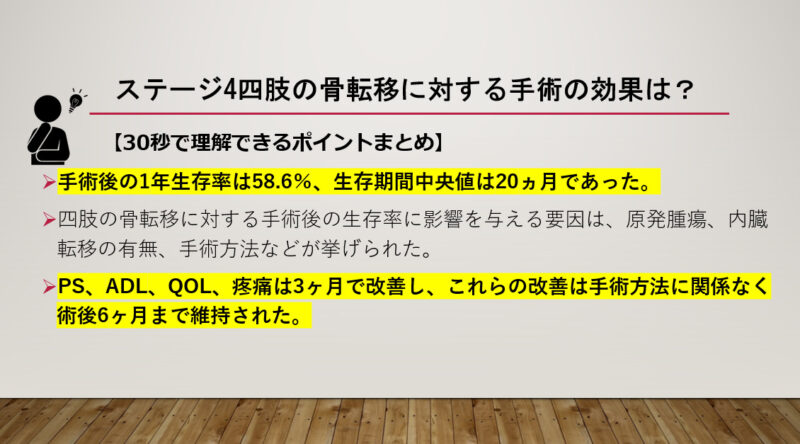
1年生存率は58.6%、生存期間中央値は20ヵ月、追跡期間中央値は12ヵ月(範囲0-130)でした。
Hara H, Sakai Y, Kawamoto T, et al. Surgical outcomes of metastatic bone tumors in the extremities (Surgical outcomes of bone metastases). J Bone Oncol. 2021 Feb 19;27:100352 J Orthop Surg Res. 2021 Jul 3;16(1):423
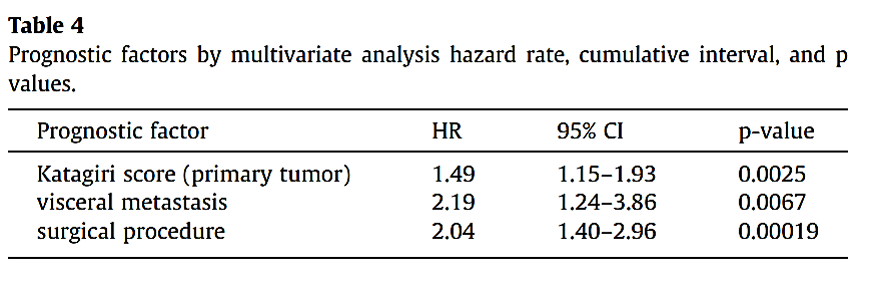
こちらの表は生存率に影響を与える因子を抽出した結果です。
原発巣の種類、内臓転移、手術方法が独立した予後因子であることが明らかになりました。
特に、”rapid growth” Katagiriサブグループに属する患者、内臓転移を有する患者、および内固定術のみを受けた患者は、他の患者に比べて予後不良でした。。
47人の整体師全員が「整体対決で負けた」枕!【Cure:Re THE MAKURA】
Hara H, Sakai Y, Kawamoto T, et al. Surgical outcomes of metastatic bone tumors in the extremities (Surgical outcomes of bone metastases). J Bone Oncol. 2021 Feb 19;27:100352 J Orthop Surg Res. 2021 Jul 3;16(1):423
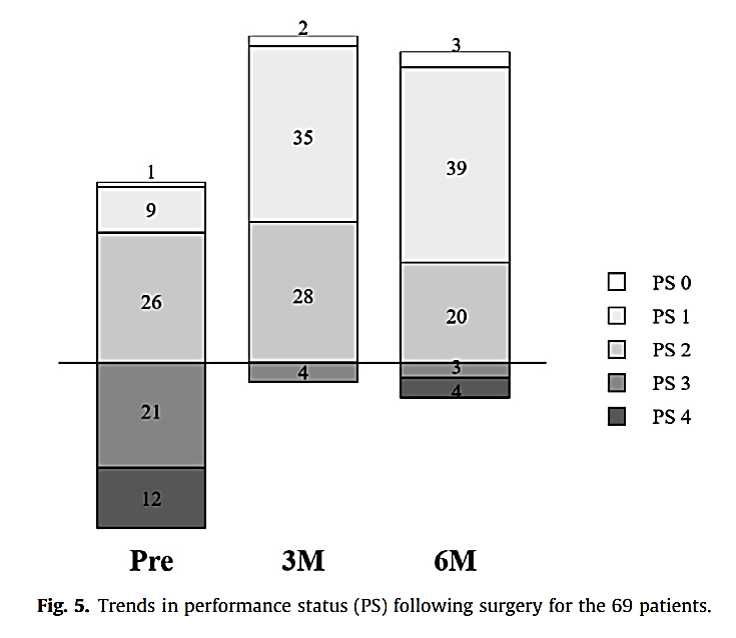
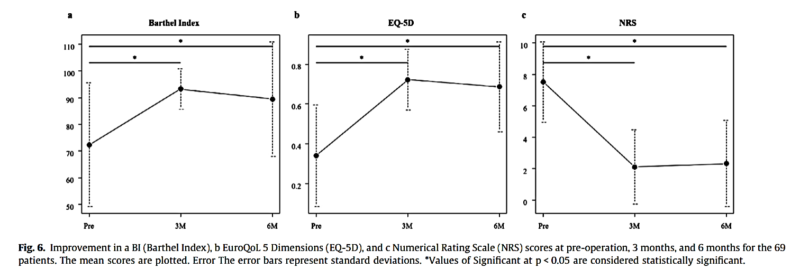
さらに、術後6ヶ月以上の経過観察を行った69例では、PS、ADL(BI)、QOL(EQ-5D)、疼痛(NRS)が術前値と比較して術後3ヶ月、6ヶ月に改善していました。
47人の整体師全員が「整体対決で負けた」枕!【Cure:Re THE MAKURA】結論
In summary, significant factors affecting survival after surgical treatment for bone metastases included the primary tumor, presence of visceral metastases, and internal fixation without tumor resection or curettage. PS, ADL, QOL, and pain improved at 3 months and these improvements were maintained until 6 months after surgery regardless of surgical procedure. It is important that the most appropriate surgical treatment, based on several factors including patient prognosis, local tumor control, and the likelihood of postoperative complications, should be provided for patients with bone metastases. We think that surgery using a tumor prosthesis after irradiation should be aware for postoperative complications. We recommend that the management of bone metastases be decided by a multidisciplinary team.
Hara H, Sakai Y, Kawamoto T, et al. Surgical outcomes of metastatic bone tumors in the extremities (Surgical outcomes of bone metastases). J Bone Oncol. 2021 Feb 19;27:100352 J Orthop Surg Res. 2021 Jul 3;16(1):423
骨転移に対する外科治療後の生存率に影響を与える有意な要因は、原発腫瘍、内臓転移の有無、腫瘍切除や掻爬を伴わない内固定術などでした。
PS、ADL、QOL、疼痛は3ヶ月で改善し、これらの改善は手術方法に関係なく術後6ヶ月まで維持されました。
骨転移患者に対しては,患者の予後,局所腫瘍制御,術後合併症の可能性などいくつかの要因を考慮した上で,最も適切な手術療法を行うことが重要です。
照射後の腫瘍プロテーゼを用いた手術は、術後合併症に注意すべきと考える。骨転移の管理は集学的なチームで決定することを推奨する。
手術の適応に関しては、原発や転移、手術方法などを考慮する必要があるので主治医に判断してもらうしかないですが、適応があれば手術を行った方がPSやADL、QOL、疼痛など多くの面で効果が期待できるようなので、検討する価値はあるようですね。
47人の整体師全員が「整体対決で負けた」枕!【Cure:Re THE MAKURA】・手術後の1年生存率は58.6%、生存期間中央値は20ヵ月であった。
・四肢の骨転移に対する手術後の生存率に影響を与える要因は、原発腫瘍、内臓転移の有無、手術方法などが挙げられた。
・PS、ADL、QOL、疼痛は3ヶ月で改善し、これらの改善は手術方法に関係なく術後6ヶ月まで維持された。
・適応があれば手術を行った方がPSやADL、QOL、疼痛など多くの面で効果が期待できるようなので、検討する価値はあると思われる。
このブログは、ガイドラインや論文などの根拠をもとに情報を発信していく予定です。
しかし、がんの病態や治療方法によっては、お読みになっているがん患者さんにはその情報が当てはまらない場合もあります。
記事の内容を参考に新しく何かを始める場合には、担当の医師や医療従事者にご確認いただくようお願いいたします。

















最近のコメント