
今回は、骨転移がある人がの運動実施可能性について調査した最新のレビューを紹介します。
がん患者さんのリハビリや運動を行う際に、リスク管理として最も注意しなければならないものの一つが骨転移になります。
がん患者さんは運動を行うべきですが、リスク管理をしっかりと行う必要があるのでしたね。
特に骨転移は骨折のリスクなどがあるので注意が必要です。
しかし、骨転移患者さんでも骨折等に注意して運動を行うことは必要と言われています。
ガイドラインでも骨転移患者さんの運動について言及されています。
そこで今回は、骨転移がある人の運動実施可能性について調査した最新のレビューを紹介します。
今回紹介する研究の概要
今回紹介する論文は、骨転移がある人の運動実施可能性について調査した内容になっています。
「Weller S, Hart NH, Bolam KA, et al. Exercise for individuals with bone metastases: A systematic review. Crit Rev Oncol Hematol. 2021 Oct;166:103433」、2021年に発行された最新のレビューです。
「ABC Cooking Studio」から生まれた女性専用フィットネスジム【Bodies】対象
Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) (Moher et al., 2009) reporting guidelines were followed and registration with PROSPERO (CRD42019121958). Electronic databases (MEDLINE, Embase, Pubmed, CINAHL, PEDro and CENTRAL) were searched from inception to 16 July 2020, using a search strategy developed in consultation with a university librarian. Additionally, grey literature and reference lists of eligible papers were searched. The search included subject headings or keywords for “cancer” and “bone metastases or advanced cancer” and “exercise” (eSupplement eTable 1). Limits included human participants and publication in English.
Inclusion criteria were: 1) design: RCT or controlled clinical trial; 2) population: 18-years or older with a diagnosis of cancer; sample included participants with metastatic bone disease (with confirmed number of participants with bone metastases); 3) intervention: any exercise intervention comprising more than one session of structured exercise; 4) comparator group: usual care, control or comparator interventions; and 5) outcome: at least one outcome related to efficacy on physical function (e.g., sit to stand), functional capacity (e.g., cardiopulmonary exercise test), muscular strength (e.g., one repetition maximum) or treatment side effect (e.g., fatigue). Exercise was operationally defined as aerobic, resistance or flexibility exercise, sports-specific training (e.g., soccer), yoga, tai chi, Pilates or a combination of any of these modalities. Structured exercise refers to an exercise prescription given to be performed in a supervised or unsupervised setting.
Weller S, Hart NH, Bolam KA, et al. Exercise for individuals with bone metastases: A systematic review. Crit Rev Oncol Hematol. 2021 Oct;166:103433
対象となる論文を電子データベース(MEDLINE,Embase,Pubmed,CINAHL,PEDro,CENTRAL)を用いて,2020年7月16日まで検索を行っています。
検索対象は、「がん」と「骨転移または進行がん」、「運動」の件名見出しまたはキーワードとしています。
ヒトを対象とし、英語での発表であることを条件となっています。
基準は1)研究デザイン: ランダム化比較試験または対照臨床試験、2)対象者:18 歳以上のがん診断者。3)介入:1セッション以上の運動介入、4)比較対象群:通常ケア、コントロールまたは比較対象の介入、5)結果:身体機能または筋力に関する有効性に関して分析していることとなっています。
運動は、有酸素運動、抵抗運動、柔軟運動、スポーツ特化型トレーニング(サッカーなど)、ヨガ、太極拳、ピラティス、またはこれらの組み合わせとされています。
最終的に17編の論文をレビューしています。
「ABC Cooking Studio」から生まれた女性専用フィットネスジム【Bodies】結果
All but one trial reported on adverse events (AEs) (Bourke et al., 2011), with nine (53%) trials measuring AEs in both intervention and comparator groups and seven (41%) trials measuring AEs in the intervention group only (Table 2). Seven (41%) trials reported use of a comprehensive classification tool that specified AE grade and severity (e.g., National Cancer Institute Common Terminology Criteria for Adverse Events). Overall, three trials (18%) reported serious adverse events (SAEs) associated with the trial and all included samples with and without bone metastases (Bjerre et al., 2019a, b; Solheim et al., 2017; Uth et al., 2014, 2016a, b). A total of 57 SAEs were reported in these three trials; 27 SAEs occurred in intervention group participants and 30 SAEs occurred in control group participants. Only four SAEs (0.5% of total exercise intervention participants) were attributed to an exercise intervention, all of which were attributed to soccer and were not related to bone metastases. One trial by Uth et al. reported three SAEs that included two fibula fractures and one partial achilles tendon rupture (Uth et al., 2014, 2016a, b). A second trial by Bjerre et al. reported 33 SAEs resulting in hospital admission, 11 in the intervention group and 22 in the usual care group, with one SAE attributed to the intervention, which was a soft-tissue injury that was not related to bone metastases (Bjerre et al., 2019a, b). Of note, in the four trials that exclusively included individuals with bone metastases, no SAEs occurred during the trials (Cormie et al., 2013; Galvão et al., 2018; Rief et al., 2014a, b, c, d, 2016; Sprave et al., 2019). Additionally, one trial reported specifically on the presence of pathological fractures and found no significant differences between the intervention and control groups at baseline (23% vs 30%, p = 0.56) or end of intervention (23% vs 30%, p = 0.59%) (Rief et al., 2014a, b, c, d, 2016).significantly.
Weller S, Hart NH, Bolam KA, et al. Exercise for individuals with bone metastases: A systematic review. Crit Rev Oncol Hematol. 2021 Oct;166:103433
まずは安全性に関する結果です。
1 件を除くすべての試験で有害事象が報告され、、9 件(53%)の試験で介入群および比較対照群の両方、7 件(41%)で介入群のみの 有害事象が報告されています。
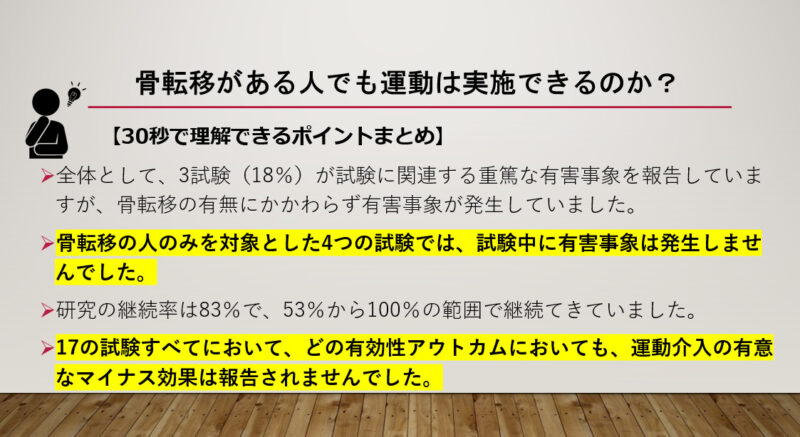
全体として、3試験(18%)が試験に関連する重篤な有害事象を報告していますが、骨転移の有無にかかわらず有害事象が発生していました。
運動介入に起因する有害事象は4件(運動介入参加者全体の0.5%)のみで、いずれもサッカーに起因し、骨転移とは関連がありませんでした。
1つの試験では、2つの腓骨骨折と1つのアキレス腱部分断裂を含む3つの有害事象が報告され、他の試験では、骨転移とは無関係の軟部組織損傷がありました。
骨転移を有する個人のみを対象とした4つの試験では、試験中に有害事象は発生しませんでした。
さらに、1つの試験では、病的骨折の有無について介入群と対照群の間に有意差は認められませんでした。
Weller S, Hart NH, Bolam KA, et al. Exercise for individuals with bone metastases: A systematic review. Crit Rev Oncol Hematol. 2021 Oct;166:103433
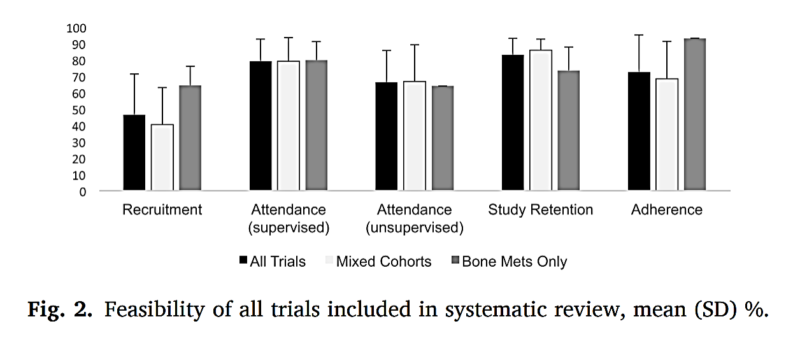
続いて実現可能性についての結果です。
全体として、平均採用率は46%で、12%から93%の範囲でした。
骨転移の人に限定された試験では、64(12)%の平均加入率が報告されました。
研究期間中の継続率は83%で、53%から100%の範囲でした。
骨転移のある人に限定された研究では、74%の継続率が報告されています。
Across all 17 trials, no significant negative effects of the exercise intervention were reported in any efficacy outcome (Table 1, eSupplement eTable 2). A variety of patient reported outcomes and objective test measures were used. A summary of the between-group efficacy results of each trial is shown in eSupplement eFig. 2. Significant between group improvement in physical function, fatigue and quality of life that favour exercise was reported in seven (54%) trials (Bourke et al., 2011; Cheville et al., 2019; Cormie et al., 2013; Galvão et al., 2018; Rief et al., 2014a, b, c, d, 2016; Villumsen et al., 2019; Yee et al., 2019), three (23%) trials (Bourke et al., 2011, 2014; Yee et al., 2019) and four (31%) trials (Bourke et al., 2014; Cheville et al., 2019; Dawson et al., 2018; Yee et al., 2019), respectively. Significant between group improvements in body composition and objective measures of muscular strength that favour exercise was reported in six (43%) trials (Cormie et al., 2013; Dawson et al., 2018; Rief et al., 2014a, b, c, d, 2016; Rosenberger et al., 2017; Solheim et al., 2017; Uth et al., 2014, 2016a, b) and six (67%) trials (Bourke et al., 2011; Cormie et al., 2013; Dawson et al., 2018; Galvão et al., 2018; Rosenberger et al., 2017; Uth et al., 2014, 2016a, b), respectively. Finally, significant between group reductions in pain that favour exercise was reported in two (29%) trials (Cheville et al., 2019; Rief et al., 2014a, b, c, d, 2016).
In trials that exclusively included individuals with bone metastases (n = 4), results were mixed and a range of test measures were used (eSupplement eTable 2). Three (75%) trials (Cormie et al., 2013; Galvão et al., 2018; Rief et al., 2014a, b, c, d, 2016) reported significant between-group improvements in physical functioning that favour exercise and two (50%) trials (Cormie et al., 2013; Galvão et al., 2018) reported significant between-group improvements in muscle strength that favour exercise. All trials measured pain (n = 4), with one (25%) trial (Rief et al., 2014a, b, c, d, 2016) reporting a reduction in pain levels and three (75%) trials (Cormie et al., 2013; Galvão et al., 2018; Sprave et al., 2019) reporting no difference between groups. No significant between group exercise effect was reported for fatigue (n = 4) or quality of life (n = 3) (Cormie et al., 2013; Rief et al., 2014a, b, c, d 2016; Sprave et al., 2019).
Weller S, Hart NH, Bolam KA, et al. Exercise for individuals with bone metastases: A systematic review. Crit Rev Oncol Hematol. 2021 Oct;166:103433
17の試験すべてにおいて、どの有効性アウトカムにおいても、運動介入の有意なマイナス効果は報告されませんでした。
身体機能、疲労、QOLの有意な群間改善が7試験(54%)で報告されています。
身体組成および筋力の客観的測定における有意な群間改善は、6(43%)の試験で報告されました。
有意な痛みの群間減少が2件(29%)の試験で報告されました。
「ABC Cooking Studio」から生まれた女性専用フィットネスジム【Bodies】結論
In the existing literature examining exercise in people with bone metastases, exercise appears to be safe and feasible, when it includes an element of supervised exercise instruction delivered by qualified exercise professionals. More research is needed to understand the magnitude of effect that exercise can achieve in this population.
Weller S, Hart NH, Bolam KA, et al. Exercise for individuals with bone metastases: A systematic review. Crit Rev Oncol Hematol. 2021 Oct;166:103433
骨転移者における運動を検討するレビューでは、専門家の監督下での運動指導の要素を含む場合、運動は安全で実行可能のようでした。
運動の効果も期待できるようですが、その効果の大きさを明らかにするために、さらなる研究が必要です。
やはり、骨転移があることを理解したうえで適切な運動を行うことは安全で効果的なようですね。
骨転移の部位や症状、治療の効果を理解する必要がありますし、
皆さんが気になる注意すべき動作などについても今後紹介していきたいと思います。
「ABC Cooking Studio」から生まれた女性専用フィットネスジム【Bodies】・全体として、3試験(18%)が試験に関連する重篤な有害事象を報告していますが、骨転移の有無にかかわらず有害事象が発生していました。
・骨転移の人のみを対象とした4つの試験では、試験中に有害事象は発生しませんでした。
・研究の継続率は83%で、53%から100%の範囲で継続てきていました。
・17の試験すべてにおいて、どの有効性アウトカムにおいても、運動介入の有意なマイナス効果は報告されませんでした。
・今まで紹介した骨転移の治療や症状を理解した上で、適切な運動を行うことは安全で効果的なようです。注意すべき動作などについては、また紹介します。
このブログは、ガイドラインや論文などの根拠をもとに情報を発信していく予定です。
しかし、がんの病態や治療方法によっては、お読みになっているがん患者さんにはその情報が当てはまらない場合もあります。
記事の内容を参考に新しく何かを始める場合には、担当の医師や医療従事者にご確認いただくようお願いいたします。















最近のコメント