今までは、運動を実施してもリンパ浮腫が増悪せずに、運動機能が改善できますよ~といった内容の論文を紹介してきました。
それでは、リンパ浮腫を増悪させないではなくて、予防するためにはどうしたらいいのでしょうか?
こんなことをした方が、リンパ浮腫が発症しにくくなるよっていうのがわかれば、とても参考になりますよね。
運動を行うことでリンパ浮腫が発症しにくくなればとても素晴らしいことです。
そこで今回は、乳がん術後の患者さんに対して、術後早期から理学療法を実施することがリンパ浮腫発症を予防できるかを検証した論文を紹介します。
スーパーフードの【モリンガプロテイン】
今回紹介する論文の概要
今回紹介する論文は、乳がん術後の患者さんに対して、術後早期から理学療法を実施することがリンパ浮腫発症を予防できるかを検証した内容になっています。
「Torres Lacomba M, Yuste Sánchez MJ, Zapico Goñi A, et al. Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer: randomised, single blinded, clinical trial. BMJ. 2010 Jan 12;340:b5396」
2010年に発行された論文です。
口腔粘膜でスポーツ遺伝子を調べる【DNA EXERCISE】
対象
対象は2005年5月から2007年6月にかけて、マドリードのプリンシペデアストゥリアス病院で、腋窩リンパ節郭清を伴う片側乳がん手術後の女性120名です、
腋窩リンパ節郭清を行わない女性、両側乳癌、全身性疾患、局所再発、理学療法に禁忌のある女性は除外しています。
「マットレスを超えるマットレス」エアツリーマットレス
介入方法
対象者を早期理学療法と教育戦略(早期理学療法群)または教育戦略のみ(対照群)を行う2群に分けて調査を行っています。
介入の時期は、術後4週、術後3ヶ月、6ヶ月、12ヶ月の4回のフォローアップを行っています。
それぞれ3回/週の頻度で、3週間の介入を行いました。
早期理学療法群の介入内容は、術後浮腫の治療に用いられる用手的リンパドレナージ(胸部、乳房、腋窩、患側上腕部)、瘢痕に対するマッサージ、肩~胸周囲のストレッチ運動、PNFといった特殊な神経や筋を促通するような運動を行っています。
さらに、自宅で1日1回、肩の運動とストレッチも実施しています。
そして、両群に教育的な介入も実施しています。
具体的には、リンパ浮腫の病態、リンパ浮腫増悪の原因、リンパ浮腫予防のための注意点などをパンフレットを使用して指導しています。
外傷や損傷の回避、感染の予防、腕の締め付けの回避、腕の使用と運動などを指導しているようですね。
【クーポンが豊富!】お得なEPARKリラク&エステ
結果
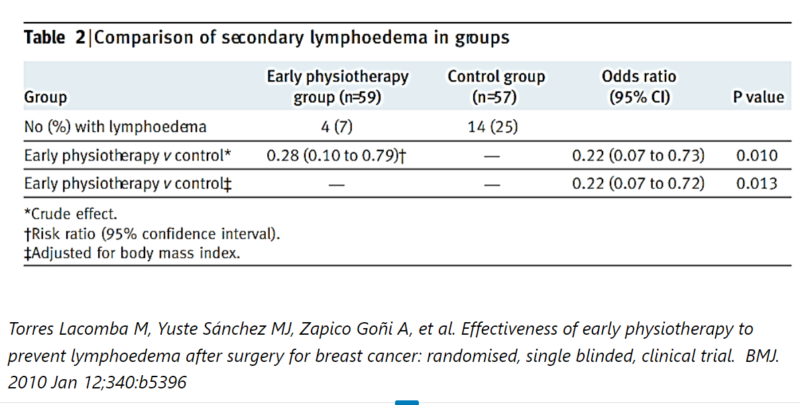
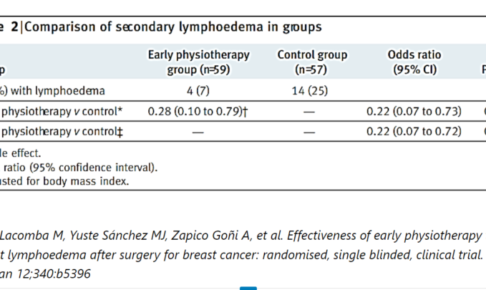
Torres Lacomba M, Yuste Sánchez MJ, Zapico Goñi A, et al. Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer: randomised, single blinded, clinical trial. BMJ. 2010 Jan 12;340:b5396
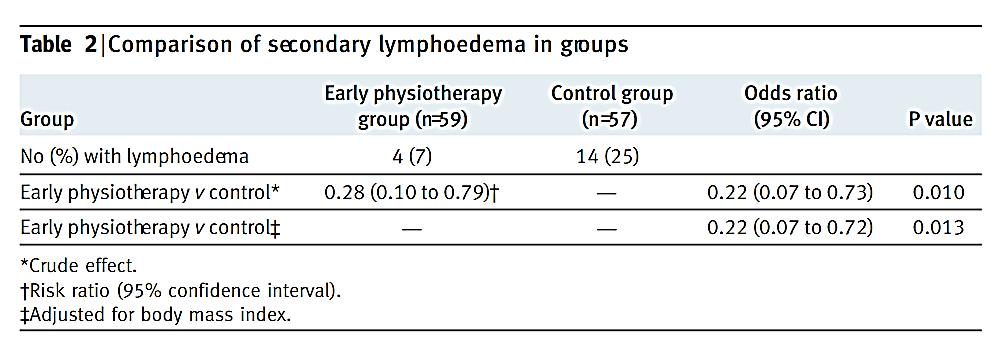
こちらの表は、12か月後のリンパ浮腫の発症率を示しています。
対照群が14名(25%)リンパ浮腫が発症したのに対して、早期理学療法群は4名(7%)しか発症していませんでした。
対象者の基本情報をBMIで調整しても、早期理学療法群の方が有意に発症率が低い結果でした。
つまり、BMIの数値に関係なく、早期理学療法を行った方がリンパ浮腫が発症しにくいということです。
Xserverドメイン
Torres Lacomba M, Yuste Sánchez MJ, Zapico Goñi A, et al. Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer: randomised, single blinded, clinical trial. BMJ. 2010 Jan 12;340:b5396
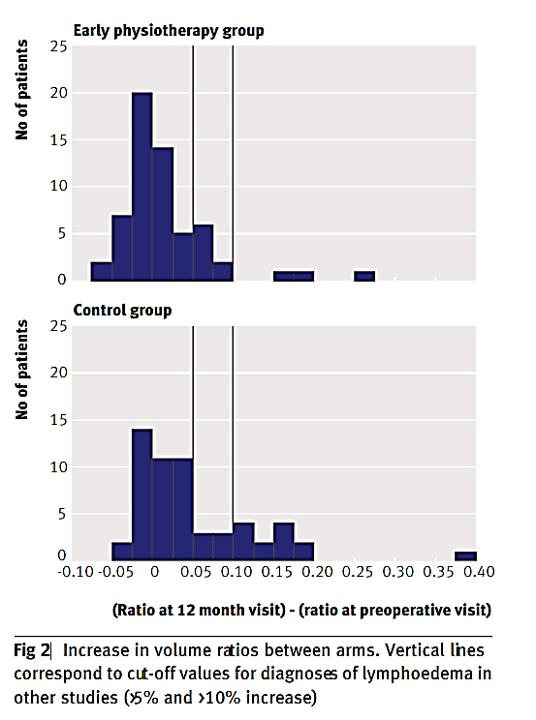
こちらの図は両群の上肢の体積の変化率を示しています。
上の図が早期理学療法群、下の図が対照群です。
グラフが右に寄るほど、上肢の体積が増加、つまりリンパ浮腫が増大しているということになります。
対照群の方がグラフが右寄りになっているので、リンパ浮腫が増大した方が多いという結果ですね。
24時間ボディメイク【マッスルプレス】
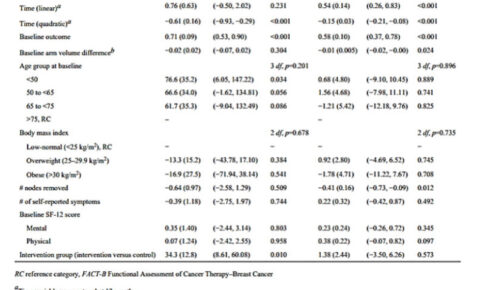
Torres Lacomba M, Yuste Sánchez MJ, Zapico Goñi A, et al. Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer: randomised, single blinded, clinical trial. BMJ. 2010 Jan 12;340:b5396

こちらの図は両群の上肢の周径の変化率を示しています。
先ほどと同じように、上の図が早期理学療法群、下の図が対照群で、グラフが右に寄るほど、上肢の周径が増加、つまりリンパ浮腫が増大しているということになります。
対照群の方が少しグラフが右寄りになっているので、リンパ浮腫が増大した方が多いという結果ですね。
自宅で快適なトレーニングをするなら!【NUOBELL】
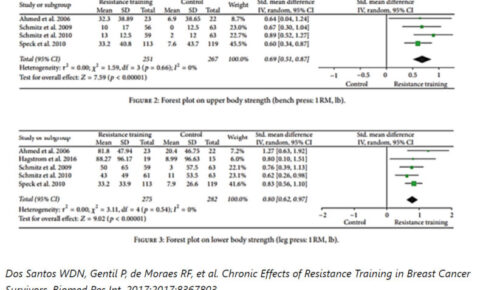
Torres Lacomba M, Yuste Sánchez MJ, Zapico Goñi A, et al. Effectiveness of early physiotherapy to prevent lymphoedema after surgery for breast cancer: randomised, single blinded, clinical trial. BMJ. 2010 Jan 12;340:b5396
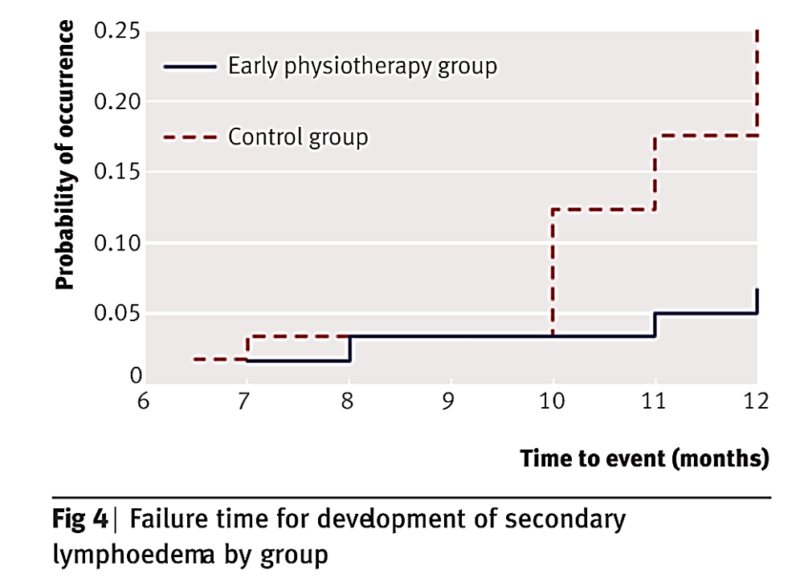
こちらの図は横軸が時間、縦軸がリンパ浮腫の発症率のグラフです。
つまり、どの時間帯でリンパ浮腫が発症したのかを示すグラフになります。
これを見ると、手術後10ヶ月くらいまでは、両群にあまり差はないですが、10か月を超えてから、急に対照群のリンパ浮腫発症が多くなっています。
早期理学療法を行うと、手術後10か月以降のリンパ浮腫が抑えられるかもしれないというわけですね。
今話題のエクオール「女性特有の悩みゆらぎをサポート」キレイ・デ・エクオール
結論
腋窩リンパ節郭清を伴う乳がん手術後の患者において、早期の理学療法は、少なくとも術後1年間はリンパ浮腫の予防と軽減に役立つと考えらました。
乳がん術後の早期の理学療法が、長期的に二次性リンパ浮腫の予防に有効であるかどうかを明らかにするために、さらなる研究が必要とのことです。
手術後の3週間×4回=12週間の理学療法と教育的な介入で、とりあえず12か月間はリンパ浮腫の発症が抑えられるようです。
教育的な介入は両群とも実施していますので、リンパ浮腫が発症しなかったのは、日常生活で注意していただけでなく、理学療法の影響もありそうですね。
ただし、リンパ浮腫は生涯発症するリスクがあるので、手術後1年だけでなく、それ以降も理学療法の効果が持続するのかを調査してほしいですね。
[ヨガ・フィットネス]欲しいウェア必ず見つかる♪【Puravida!】
・早期理学療法と教育的介入を行ったところ、教育的介入を行っただけの対照群よりも12か月後のリンパ浮腫発症率が低かった。
・早期理学療法を行うことで、とりあえず手術後12か月間のリンパ浮腫発症のリスクは軽減するかもしれないが、長期間の効果に関しては今後検証が必要である。
このブログは、ガイドラインや論文などの根拠をもとに情報を発信していく予定です。
しかし、がんの病態や治療方法によっては、お読みになっているがん患者さんにはその情報が当てはまらない場合もあります。
記事の内容を参考に新しく何かを始める場合には、担当の医師や医療従事者にご確認いただくようお願いいたします。















最近のコメント