最近はがん患者の骨粗鬆症について紹介しています。
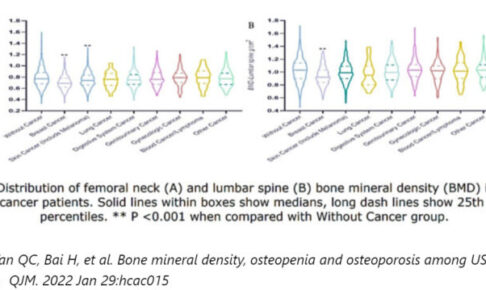
乳がん、泌尿器がん、皮膚がん、肺がん、婦人科がんなどが骨密度が低下しやすいんでしたね。
そして、がん治療に伴う骨量低下に対して、どのように管理すればいいかも紹介させていただきました。。

ホルモン治療を行っているがん患者さんは、骨密度を評価して、骨密度に応じて骨粗鬆症の治療を行うことが推奨されていました。
ホルモン治療といえば、乳がんと前立腺がんの患者さんになりますね。
それでは、ホルモン治療を行っているがん患者さんは実際にどの程度骨密度が低下しているのでしょうか?
今回は、ホルモン治療を行っている前立腺がん患者さんの骨密度低下について調査した論文を紹介いたします。
・骨密度に影響を与える要因は年齢、糖尿病、BMI、レントゲンでの脊椎骨折、ADTの治療期間、BAPが挙げられた。
・ADTの治療期間が長くなるにつれて、骨密度が低下し、骨粗鬆症の有病率が増加する。
・今回の研究では6年以上治療している患者さんは骨粗鬆症の有病率が45%であった。
・数年間治療を継続している方は骨密度に注意したほうがよい。
今回紹介する研究の概要
今回紹介する論文は、婦ホルモン治療を行っている前立腺がん患者さんの骨密度低下について調査した内容になっています。
「Kato S, Kawase M, Kato D, et al. Decrease of bone mineral density in Japanese patients with non-metastatic prostate cancer treated with androgen deprivation therapy. J Bone Miner Metab. 2019 Jan;37(1):72-80」、2019年に発行された日本で研究された論文です。
必須アミノ酸とグリシンで理想のカラダを目指すアミノ酸サプリ「アミノスパルタンGOLD」対象
Consecutive Japanese male patients with NMPC who attended our institution from January 2011 to November 2016 who were receiving continuous ADT or who were planning to receive ADT (hormone naive) were enrolled in this study. All of their prostate cancers had been proven pathologically by needle biopsy, and imaging tests (computed tomography, magnetic resonance imaging, and bone scintigraphy) revealed no metastatic lesions. ADT included gonadotropin-releasing hormone agonists (GnRHa) or combinations of GnRHa and anti-androgens. Patients receiving intermittent ADT and patients with castration-resistant prostate cancer were excluded. Moreover, patients with bone metabolic disease, including Paget’s disease, osteomalacia, hyperprolactinemia, hyper- or hypothyroidism, hyperparathyroidism, and Cushing disease, or previous or concomitant treatment with bone-modifying agents, including bisphosphonates, denosumab, parathyroid hormones, selective estrogen receptor modulators, calcitonin, and calcitriol, were excluded from the study. The study protocol was approved by the local institutional review board.
Kato S, Kawase M, Kato D, et al. Decrease of bone mineral density in Japanese patients with non-metastatic prostate cancer treated with androgen deprivation therapy. J Bone Miner Metab. 2019 Jan;37(1):72-80
対象の条件は、2011年1月から2016年11月までに通院して、アンドロゲン除去療法(ADT)を受けている、もしくは受ける予定の非転移性前立腺がん患者さん230名となっています。
骨密度に関係しそうな合併症があったり、治療を行っている患者さんは除外されています。
具体的には、パジェット病、甲状腺機能亢進症または甲状腺機能低下症、副甲状腺機能亢進症、およびクッシング病を含む骨代謝性疾患の患者など。
ビスフォスフォネート、デノスマブ、副甲状腺ホルモン、選択的エストロゲン受容体モジュレーター、カルシトニン、およびカルシトリオールといった骨修飾薬を使用された患者さんが除外されています。
必須アミノ酸とグリシンで理想のカラダを目指すアミノ酸サプリ「アミノスパルタンGOLD」方法
BMD of the posteroanterior (PA) spine (L2–L4) and non-dominant femoral neck was measured using dual-energy X-ray absorptiometry (DEXA). DEXA was performed using QDR-Discovery (Hologic, Inc., Marlborough, MA, USA). T-scores and young mean adult (YAM) values were calculated using the Hologic database for East Asian ethnicity. The coefficient of variation of BMD at our institution was 1.0% at both the PA spine and total hip. X-ray examinations of the PA spine and lateral spine (cervical, thoracic, lumbar) were performed to assess the presence of silent vertebral fractures. To assess patient characteristics, medical records and questionnaires were investigated to check whether they had any factors that possibly affected BMD such as body mass index (BMI), previous bone fractures of the spine or hip, any bone fractures during ADT, family history of bone fractures of the spine or hip, smoking status, alcohol excess, hypertension, diabetes, rheumatoid arthritis, chronic kidney disease (CKD) and steroid administration. Bone metabolism markers, bone alkaline phosphatase (BAP) as a bone formation marker, and urine type I collagen cross-linked N-telopeptide (urine NTx) or tartrate-resistant acid phosphatase 5b (TRACP-5b) as bone resorption markers were also measured to assess bone metabolism. Urine specimens for measuring urine NTx were obtained in the morning.
Kato S, Kawase M, Kato D, et al. Decrease of bone mineral density in Japanese patients with non-metastatic prostate cancer treated with androgen deprivation therapy. J Bone Miner Metab. 2019 Jan;37(1):72-80
二重エネルギーX線吸収測定法(DEXA)を使用して、腰椎と大腿骨の骨密度を測定しています。
そして、T-スコアと若年平均成人(YAM)値を算出しています。
これらの数値を用いて、骨量減少や骨粗鬆症の診断ができるんでしたね。
他の調査項目としては、圧迫骨折の有無を確認するための脊椎レントゲンを撮影しています。
そして、BMIや骨折歴、家族の骨折歴、喫煙、飲酒、高血圧、糖尿病、関節リウマチ、慢性腎臓病、ステロイドの使用に関しても聴取しています。
骨形成マーカーとしてBAP、骨吸収マーカーとしてNTx、TRACP-5bという骨代謝マーカーを測定しています。
骨形成マーカーというのがどれくらい骨をしっかり造る能力があるのか、骨吸収マーカーというのがどれくらい骨破壊が進みやすいのかの指標となります。
必須アミノ酸とグリシンで理想のカラダを目指すアミノ酸サプリ「アミノスパルタンGOLD」結果
Kato S, Kawase M, Kato D, et al. Decrease of bone mineral density in Japanese patients with non-metastatic prostate cancer treated with androgen deprivation therapy. J Bone Miner Metab. 2019 Jan;37(1):72-80
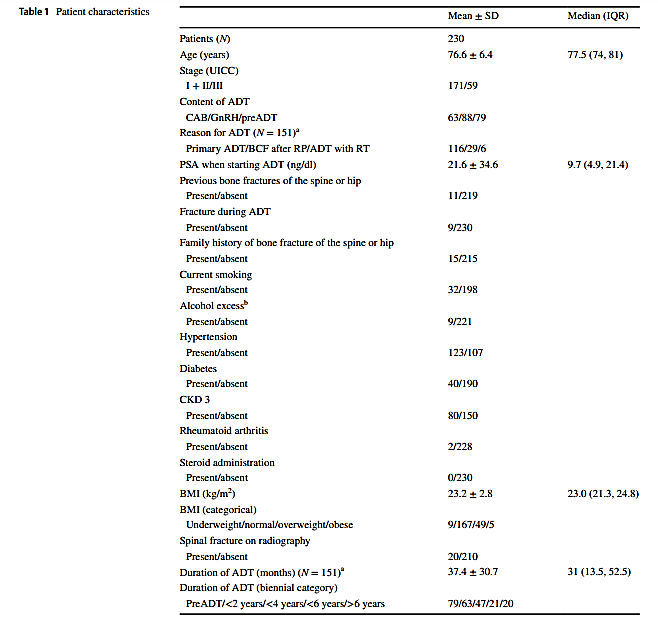
こちらの表が対象者の特徴になります。
230人の患者のうち、151人(65.7%)がADTを受けており、79人(34.4%)はまだ治療前でした。
ADTを受けていた151人の患者のADTの平均期間は37.4±30.7ヶ月でした。
ADTの治療期間は2年未満が27.4%、2〜4年が20.4%、4〜6年が9.1%、6年以上が8.7%となっています。
約3年間ほど治療を受けられているということですね。
骨折や喫煙、飲酒、リウマチ、ステロイドなんかはほとんどいませんが、高血圧や腎臓病に該当している方はそこそこいるみたいですね。
Kato S, Kawase M, Kato D, et al. Decrease of bone mineral density in Japanese patients with non-metastatic prostate cancer treated with androgen deprivation therapy. J Bone Miner Metab. 2019 Jan;37(1):72-80
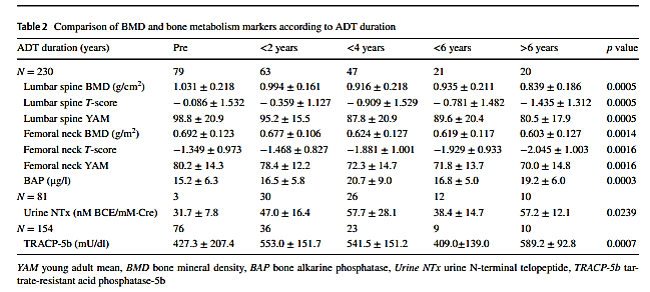
こちらの表は骨密度と骨代謝マーカーの結果をADTの治療期間別に比較しています。
ADTの治療期間が長くなると、腰椎と大腿骨の骨密度は徐々に減少しています。
骨代謝マーカーもADTの治療期間が長くなると徐々に増悪するようです。
大腿骨のYAM値をみると、治療前は80%とギリギリ正常値ですが、治療が6年間続くと70%と骨粗鬆症の数値となってしまっています。
単変量解析では、腰椎骨密度に影響を与える変数は糖尿病,BMI,脊椎骨折、ADTの期間、BAP、NTx、TRACP-5bでした。
大腿骨骨密度影響を与える変数は糖尿病、BMI、年齢、脊椎骨折、ADTの期間、BAP、NTx、TRACP-5bでした。
骨折歴、家族の骨折歴、ライフスタイ、高血圧、CKD、関節リウマチは骨密度と関係していませんでした。
骨代謝マーカーが骨密度と関連するのは当然でしょうが、BMIが低い、年齢が高い、ADTの治療期間が長い患者さんは骨密度をチェックしたほうがよさそうですね。
必須アミノ酸とグリシンで理想のカラダを目指すアミノ酸サプリ「アミノスパルタンGOLD」Kato S, Kawase M, Kato D, et al. Decrease of bone mineral density in Japanese patients with non-metastatic prostate cancer treated with androgen deprivation therapy. J Bone Miner Metab. 2019 Jan;37(1):72-80
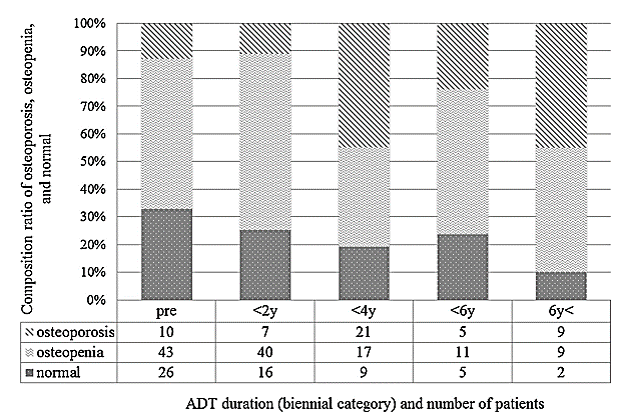
こちらは治療期間別の骨粗鬆症の有病率を示しています。
骨粗鬆症の有病率は、ホルモン未投与患者で12.7%、治療歴が2年未満の患者で11.1%、ADTが2〜4年の患者で44.7%、ADTが4〜6年の患者で23.8%、の6年以上の患者の45.0%となっています。
ADTの期間が長くなると、骨粗鬆症の有病率は上がっていく傾向があるようです。
Kato S, Kawase M, Kato D, et al. Decrease of bone mineral density in Japanese patients with non-metastatic prostate cancer treated with androgen deprivation therapy. J Bone Miner Metab. 2019 Jan;37(1):72-80
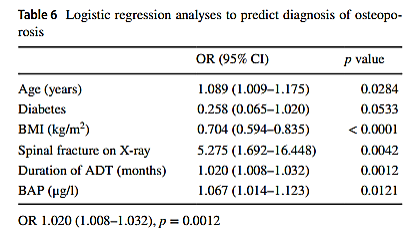
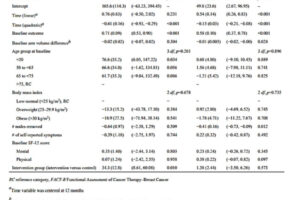
こちらの表は多変量解析という統計手法で、骨粗鬆症の要因として抽出された項目です。
上から、年齢、糖尿病、BMI、レントゲンでの脊椎骨折、ADTの治療期間、BAPが、骨粗鬆症に関連する要因として抽出されています。
やはり、ホルモン治療を長期で行うことは骨粗鬆症の発症と関係するようですね。
必須アミノ酸とグリシンで理想のカラダを目指すアミノ酸サプリ「アミノスパルタンGOLD」結論
This study showed that ADT negatively affected lumbar spine and femoral neck BMD in Japanese patients with NMPC. As the duration of ADT increased, BMD decreased at both sites. We also observed a progressive increase in the prevalence of osteoporosis in Japanese NMPC patients with ADT. The prevalence of osteoporosis reached 45% after 6 years of ADT. In addition, we investigated patient backgrounds in detail for anything that may possibly affect BMD in the Asian population, and we showed for the first time a positive relationship between BMD and diabetes in prostate cancer patients undergoing ADT. Larger scale and prospective studies are warranted to clarify ethnic differences in the prevalence of osteoporosis accompanying ADT in prostate cancer patients of Asians and Caucasians.
Kato S, Kawase M, Kato D, et al. Decrease of bone mineral density in Japanese patients with non-metastatic prostate cancer treated with androgen deprivation therapy. J Bone Miner Metab. 2019 Jan;37(1):72-80
この研究は、ADTというホルモン治療日本人の非転移性前立腺がん患者の腰椎と大腿骨頸部の骨密度に悪影響を及ぼしたことを示しました。
ADTの期間が長くなると、骨密度が減少し、骨粗鬆症の有病率が増加することが明らかになりました。
さらに、ADTを受けている前立腺癌患者の骨密度と糖尿病関係性を認めた初めての研究のようです。
ホルモン治療は長期間行う治療になってきますので、数年間治療を継続している方は骨密度に注意するようにしておいてください。
必須アミノ酸とグリシンで理想のカラダを目指すアミノ酸サプリ「アミノスパルタンGOLD」・骨密度に影響を与える要因は年齢、糖尿病、BMI、レントゲンでの脊椎骨折、ADTの治療期間、BAPが挙げられた。
・ADTの治療期間が長くなるにつれて、骨密度が低下し、骨粗鬆症の有病率が増加する。
・今回の研究では6年以上治療している患者さんは骨粗鬆症の有病率が45%であった。
・数年間治療を継続している方は骨密度に注意したほうがよい。
このブログは、ガイドラインや論文などの根拠をもとに情報を発信していく予定です。
しかし、がんの病態や治療方法によっては、お読みになっているがん患者さんにはその情報が当てはまらない場合もあります。
記事の内容を参考に新しく何かを始める場合には、担当の医師や医療従事者にご確認いただくようお願いいたします。
このブログは、ガイドラインや論文などの根拠をもとに情報を発信していく予定です。
しかし、がんの病態や治療方法によっては、お読みになっているがん患者さんにはその情報が当てはまらない場合もあります。
記事の内容を参考に新しく何かを始める場合には、担当の医師や医療従事者にご確認いただくようお願いいたします。















最近のコメント