
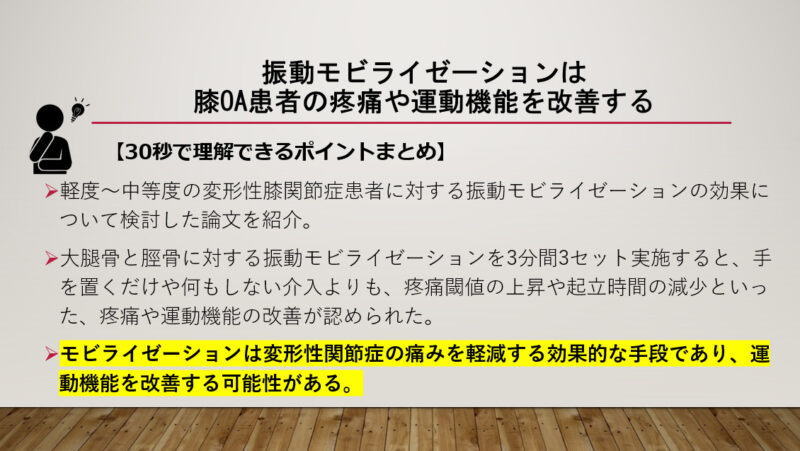
今回は、軽度~中等度の変形性膝関節症患者に対する振動モビライゼーションの効果について検討した論文を紹介します。
前回は軽症の変形性膝関節症患者に対する自転車運動や高強度のマシントレーニングの効果についてについて紹介しました。


早期の変形性膝関節症患者さんには運動は効果的なようですね。
一方で、徒手的なリハビリを行う理学療法士さんも多いですよね。
マッサージやモビライゼーションなんかは、筋肉を緩めたり、関節の動きを良くするような主義になります。
その効果はどうなのでしょうか?
今回は、軽度~中等度の変形性膝関節症患者に対する振動モビライゼーションの効果について検討した論文を紹介します。
今回紹介する研究の概要
今回紹介する論文は、軽軽度~中等度の変形性膝関節症患者に対する振動モビライゼーションの効果について検討した内容になっています。
「Moss P, Sluka K, Wright A. et al. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Man Ther. 2007 May;12(2):109-18.」、2007年に発行された少し古い論文ですね。
64万人の患者様の声から誕生した腰痛対策マットレス『ドクタータフィ』対象
Volunteers reporting mild to moderate pain from knee osteoarthritis were sought. This study also required participants to be able to walk short distances, with or without an aid. Volunteers were excluded if they had recently undergone lower limb surgery, had co-existing inflammatory or neurological conditions, experienced altered sensation around their knee, or exhibited cognitive difficulties.
Moss P, Sluka K, Wright A. et al. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Man Ther. 2007 May;12(2):109-18.
対象は変形性膝関節症による軽度から中等度の疼痛を訴える患者38名です。
参加者は、補助具の有無にかかわらず、短距離の歩行が可能であることが条件となっています。
下肢の手術を最近受けた人、炎症性疾患や神経疾患を併発している人、膝周辺の感覚に変化が見られる人、認知能力に問題がある人は、対象から除外されています。
64万人の患者様の声から誕生した腰痛対策マットレス『ドクタータフィ』方法
Pressure pain threshold (PPT) was measured using a digital pressure algometer (Somedic AB, Farsta, Sweden), in accordance with similar clinical studies (Vicenzino et al., 2001; Collins et al., 2004; Yeo and Wright, 2004). PPT has been defined as the lowest stimulus intensity at which a subject perceives mechanical pain (Vanderweeen et al., 1996). Hypoalgesia, or decreased response to mechanical pain stimuli, therefore exhibits as increased PPT.
A horizontal 10 cm visual analogue scale (VAS), with end-points marked ‘no pain’ and ‘worst pain imaginable’, was administered immediately after the timed ‘up and go’ test, before and after each experimental condition, with difference scores used for analysis.
The self-administered Western Ontario and McMaster Universities (WOMAC) knee osteoarthritis index pain subscale (Bellamy et al., 1988) was used to evaluate knee pain at baseline and in the 24 h before and after each test session.
Moss P, Sluka K, Wright A. et al. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Man Ther. 2007 May;12(2):109-18.
痛みに関して3つの評価を行っております。
圧痛閾値(PPT)を、デジタル圧痛計(Somedic AB, Farsta, Sweden)を用いて測定しています。
PPTは、被験者が機械的な痛みを感じる最低の刺激強度と定義されています(Vanderweeenら, 1996)。
したがって、痛覚減退、すなわち機械的な痛み刺激に対する反応の低下は、PPTの増加として現れます。
終点が「痛みなし」と「想像しうる最悪の痛み」である水平10cmの視覚的アナログスケール(VAS)を、Timed Up and Goテストの直後、各介入条件の前後に実施しました。
ベースライン時および各テストセッションの前後24時間における膝関節痛の評価には、自記式のWOMAC(Western Ontario and McMaster Universities)変形性膝関節症指標疼痛サブスケール(Bellamy et al.、1988)を使用しています。
64万人の患者様の声から誕生した腰痛対策マットレス『ドクタータフィ』A 3 m timed ‘up and go’ walk test (Podsiadlo and Richardson, 1991) was applied before and after each experimental condition. The test measured time taken to stand from a standard arm-less chair, briskly walk to a 3 m mark, turn and return to sit.
The self-administered WOMAC function subscale (Bellamy et al., 1988) was completed at the first session in order to provide baseline functional data. The index comprises 17 written questions, presented in Likert-scale format, identical to the pain subscale. Total possible scores range from 0 to 68, with a higher score demonstrating greater disability.
Moss P, Sluka K, Wright A. et al. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Man Ther. 2007 May;12(2):109-18.
運動機能に関して2つの評価を行っております。
各介入条件の前後にTimed Up and Goテストを実施しています。
このテストは、標準的な肘なし椅子から立ち上がり、3mの地点まで勢いよく歩き、ターンして座り直すまでの時間を計測したものです。
自記式のWOMAC機能下位尺度(Bellamyら、1988)が、ベースラインの機能データを提供するために、最初のセッションで記入されています。
64万人の患者様の声から誕生した腰痛対策マットレス『ドクタータフィ』Each subject experienced all three experimental conditions in random order over three sessions. All conditions were applied for a total of 10 min, comprising three sets of 3 min, alternating with 30-s rests. All verbal instructions and positioning were strictly standardized using a script.
①The treatment condition consisted of a large-amplitude, AP glide of the tibia on the femur (Maitland, 1990). The subject was positioned comfortably in supine, knees in slight flexion, supported on a pillow. The therapist stabilized the femur with one hand whilst applying pain-free, oscillatory glides of the proximal tibia with the other.
②The manual contact condition precisely reproduced the hand positioning of the treatment condition without applying any movement. All interactions, procedures and timings were identical.
③The no-contact control condition reproduced all interactions, procedures and timing, without applying any manual contact.
Moss P, Sluka K, Wright A. et al. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Man Ther. 2007 May;12(2):109-18.
各被験者は3回のセッションで3つの介入条件すべてを無作為の順序で経験しました。
すべての条件は、3分間の休憩を交互に3セット、合計10分間適用されています。
介入条件は以下の通りです。
①大腿骨に対する脛骨の振幅モビライゼーションを実施した。被験者は仰臥位で膝をわずかに屈曲させ、枕に支えられた状態で安楽な姿勢で、セラピストは片手で大腿骨を安定させ、もう片方の手で脛骨近位部を無痛で振動させながら滑走させます。
②治療条件の手の位置を正確に再現し、いかなる動きも加えていません。
③接触なし対照条件は、手動接触を一切行っていません。
つまり、同一対象者に①モビライゼーションを行った②手を置いただけ③何もしなかったという3つの介入を行い、その前後の反応を調査しています。
今回のモビライゼーションとは、膝周囲の骨を振動を与えるように小刻みに動かして関節の動きを良くするような手技ですね。
64万人の患者様の声から誕生した腰痛対策マットレス『ドクタータフィ』結果
Moss P, Sluka K, Wright A. et al. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Man Ther. 2007 May;12(2):109-18.
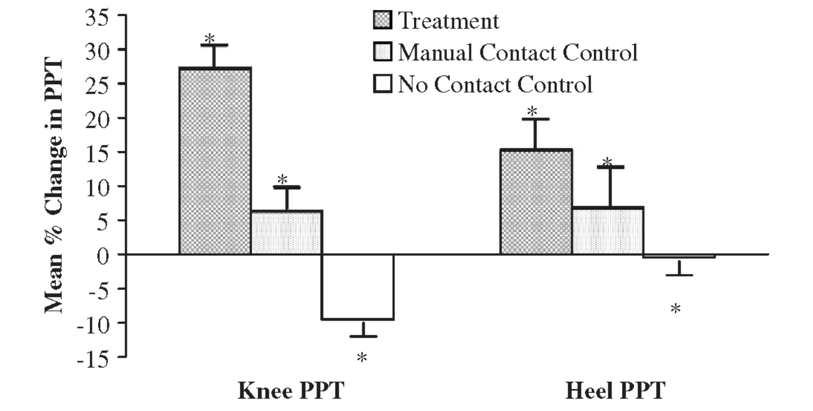
こちらは介入前後の圧痛閾値の変化です。
それぞれ左からモビライゼーション、手を置くだけ、なにもしないの介入のグラフであり、グラフが上がると閾値が高くなる、すなわち痛みに強くなるということになります。
モビライゼーションを行った方が、手を置くだけや何もしないよりも、圧痛閾値が高くなっており、痛みに強くなっていました。
Moss P, Sluka K, Wright A. et al. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Man Ther. 2007 May;12(2):109-18.
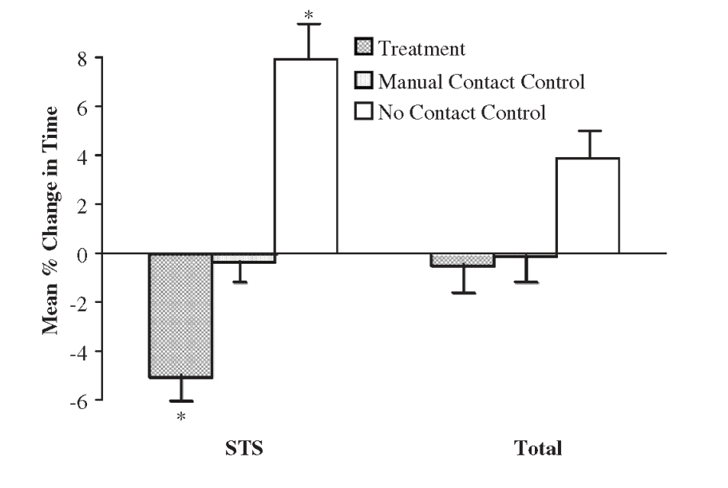
こちらは介入前後の運動機能の変化です。
それぞれ左からモビライゼーション、手を置くだけ、なにもしないの介入のグラフであり、グラフが下がると立ち座りや歩行の時間が短くなる、すなわち運動機能が上がっているということになります。
モビライゼーションを行った方が、手を置くだけや何もしないよりも、立ち座りの時間が短くなっており、運動機能が上がっていました。
64万人の患者様の声から誕生した腰痛対策マットレス『ドクタータフィ』結論
The purpose of this study was to investigate the initial effects on pain and function of lower limb joint mobilization. The study has provided new experimental evidence that accessory mobilization of a human osteoarthritic knee joint has both an immediate local and a more widespread hypoalgesic effect. This supports the response seen in animal studies (Sluka and Wright, 2001). Clinically therefore, joint mobilization may be an effective means of reducing osteoarthritic pain and may potentially improve motor function.
Moss P, Sluka K, Wright A. et al. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia. Man Ther. 2007 May;12(2):109-18.
本研究の目的は、下肢関節のモビライゼーションが痛みと機能に及ぼす初期効果を調べることです。
この結果は、即時的な局所的効果とより広範囲な鎮痛効果が得られるという証拠を提供するものです。
モビライゼーションは変形性関節症の痛みを軽減する効果的な手段であり、運動機能を改善する可能性があります。
モビライゼーションが疼痛や運動機能の改善に効果があるという結果でしたね。
私個人は運動の指導を行うことがメインですが(徒手的な技術がないので・・・)、ちゃんと研修を受けた医療者がいるのであれば、徒手的な治療を受けることも一つの手段ですね。
64万人の患者様の声から誕生した腰痛対策マットレス『ドクタータフィ』・大腿骨と脛骨に対する振動モビライゼーションを3分間3セット実施すると、手を置くだけや何もしない介入よりも、疼痛閾値の上昇や起立時間の減少といった、疼痛や運動機能の改善が認められた。
・この結果は、即時的な局所的効果とより広範囲な鎮痛効果が得られるという証拠を提供するものである。
・モビライゼーションは変形性関節症の痛みを軽減する効果的な手段であり、運動機能を改善する可能性がある。
・ちゃんと研修を受けた医療者がいるのであれば、徒手的な治療を受けることも一つの手段かもしれない。
このブログは、ガイドラインや論文などの根拠をもとに情報を発信していく予定です。
しかし、がんの病態や治療方法によっては、お読みになっているがん患者さんにはその情報が当てはまらない場合もあります。
記事の内容を参考に新しく何かを始める場合には、担当の医師や医療従事者にご確認いただくようお願いいたします。


















最近のコメント